Most employers choose a health plan by picking a carrier, selecting a network tier, and settling on a deductible level. The price they pay is whatever the carrier decides based on their negotiated rates with hospitals and physicians within that network. It is a system almost nobody fully understands, and the prices it generates bear little resemblance to the actual cost of the care delivered. A knee replacement that costs a hospital $8,000 to perform might be billed at $85,000 and settled at $42,000 through a carrier contract, and the employer has almost no visibility into any of those numbers.
Reference-based pricing works differently. Instead of tying reimbursement to carrier-negotiated rates with a specific network of providers, a reference-based pricing plan sets reimbursement at a fixed multiplier of the Medicare reimbursement rate for the same service. Employees can use nearly any provider who accepts Medicare. The plan pays a set percentage above what Medicare would pay for that procedure at that facility. The employer captures a significant portion of the gap between inflated carrier rates and what the service actually costs.
The model has been gaining traction among mid-size employers for the past decade, and it has moved firmly into the mainstream for groups with 30 to 250 employees who want an alternative to traditional PPO network arrangements. This guide explains exactly how the structure works, what the employee experience looks like in practice, where the risk points are, and how to know whether it is a reasonable fit for your company.
When your employee visits an in-network hospital or specialist, the hospital submits a bill at its chargemaster rate, which is the hospital's list price. That list price is then reduced to the carrier's contracted rate for that service at that facility. The gap between the chargemaster price and the contracted rate is called the discount. The carrier advertises that discount as a benefit of their network. Your employee sees the contracted rate as their cost basis for deductibles and cost-sharing. You, as the employer, pay the contracted rate minus whatever the employee owes.
What this system does not tell you is how the contracted rate compares to the actual cost of delivering that service. For many common procedures, carrier contracted rates run 200% to 400% above Medicare reimbursement rates for the same service at the same facility. The carrier's discount from chargemaster is real, but it starts from an inflated baseline. The net result: you are paying several times the Medicare-equivalent rate for services that cost far less to deliver, and your contract with the carrier gives you no visibility into that calculation.
Large employers with 500 or more covered employees have the leverage to negotiate carrier rates directly. They can demand claims transparency, comparison data across facilities, and actuarial analysis of their own book. For most employers with 30 to 250 employees, that level of access does not exist. You accept the carrier's standard contracted rates for your region, which are built to support the carrier's network maintenance costs and profit margins alongside your actual claims costs.
This is one reason the fully insured small and mid-size market consistently produces higher effective costs per covered life than the large-group market. The employer in the middle pays network-maintenance overhead without the data or leverage to evaluate whether that overhead is justified. Reference-based pricing removes that overhead by removing the carrier network entirely and replacing it with a transparent pricing anchor.
Medicare reimbursement rates are published by the Centers for Medicare and Medicaid Services and represent what the federal government pays providers for each procedure, by region and by facility type. These rates are not secret. They are publicly available, updated annually, and widely understood by providers. Every hospital that accepts Medicare patients, which is the overwhelming majority of hospitals in the United States, is familiar with Medicare rates for every service they provide.
A reference-based pricing plan sets its reimbursement schedule as a multiplier of these published Medicare rates. Common reimbursement levels run from 110% to 200% of Medicare, with most commercially designed plans landing between 120% and 160%. At 150% of Medicare, a service that Medicare would reimburse at $10,000 would be paid at $15,000. That is still substantially below what a carrier-contracted rate for the same service at the same hospital might be, but it is a defined, transparent, and defensible reimbursement level that most providers can work with.
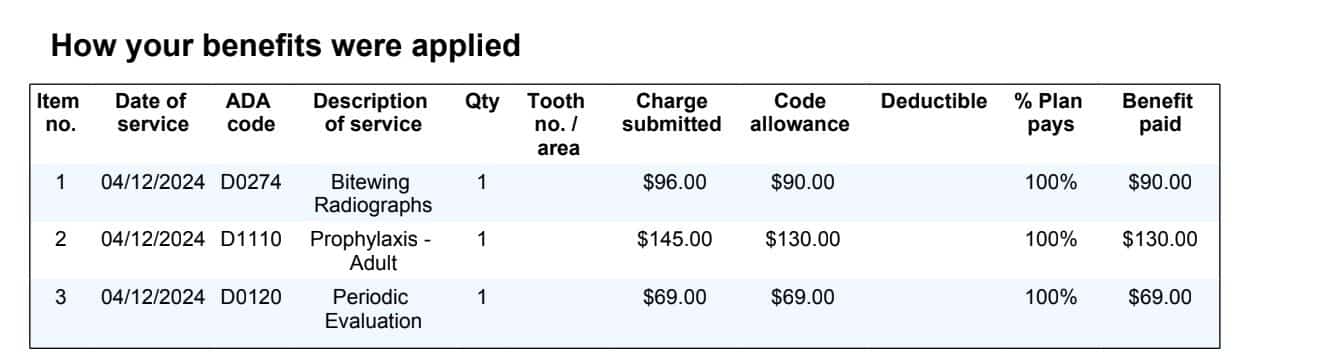
In a reference-based pricing plan, the plan administrator or third-party administrator processes each claim by identifying the Medicare reimbursement rate for that procedure code at that facility type in that region, applying the plan's multiplier, and sending payment directly to the provider at that amount. The employee receives an explanation of benefits showing what was billed, what was paid, and what if anything they owe under their deductible and out-of-pocket structure.
The employer never sees inflated chargemaster rates driving their claims costs. The third-party administrator and stop-loss carrier work from the same transparent Medicare baseline. This makes it significantly easier to audit claims, identify high-cost outliers, and understand exactly where the health plan dollars are going. For employers accustomed to receiving dense carrier reports they cannot interpret, the transparency shift alone is often valuable. You can read more about what your claims data should be telling you at What Your Health Plan's Claims Report Is Really Telling You.
Reference-based pricing plans are typically administered through independent third-party administrators rather than traditional carriers. The third-party administrator handles claims processing, member services, provider negotiations, and balance billing resolution. Stop-loss coverage, which protects the employer against catastrophic individual or aggregate claims, is placed separately through a stop-loss carrier. The employer is the plan sponsor and bears the underlying claim liability, with the stop-loss layer capping their exposure.
This structure places reference-based pricing firmly in the category of self-funded or partially self-funded health plans. The employer needs to understand their role as plan sponsor and the fiduciary responsibilities that accompany it. For a detailed explanation of self-funded plan compliance obligations, see The Compliance Shift: What Changes When Your Company Moves to a Self-Funded Plan.
One of the most common objections employers raise about reference-based pricing is employee access to providers. In a traditional PPO plan, employees are familiar with the idea of staying in-network to minimize costs. An out-of-network visit means higher out-of-pocket exposure. Reference-based pricing eliminates the network concept almost entirely. Employees can see any provider who accepts Medicare.
In most US markets, that universe of providers is large. The vast majority of hospitals, health systems, and physician practices accept Medicare patients. What reference-based pricing does not guarantee is that every provider will accept the RBP reimbursement as payment in full. That is where the balance billing question becomes important.
Balance billing occurs when a provider receives the RBP payment, determines it is less than their expected rate, and sends the patient a separate bill for the difference. This is the primary risk in a reference-based pricing arrangement, and it is the factor that makes plan design and third-party administrator selection more important than in a traditional network plan.
A well-designed RBP plan includes several layers of balance billing protection. First, the third-party administrator or a dedicated advocacy organization typically contacts providers before or immediately after services to explain the plan's reimbursement model and negotiate acceptance. Second, if a provider pursues the member for a balance bill, the plan provides legal representation and dispute resolution services. Third, some plans include a member hold-harmless provision, which means the plan guarantees the member will not ultimately pay any balance-billed amount beyond their normal cost-sharing, with the plan and administrator handling the dispute at no additional cost to the member.
Balance billing rates vary significantly by geography and provider type. Large health systems with strong market positions in concentrated markets tend to be less willing to accept RBP reimbursement and more likely to pursue balance billing. Smaller independent hospitals, rural facilities, and practice groups are often more accommodating. A third-party administrator that specializes in RBP administration will typically have a track record with providers in your area and can steer members toward facilities that have a clean history of accepting the reimbursement model.
Reference-based pricing shifts some responsibility to employees that a traditional network plan handles silently. In a PPO plan, the in-network vs out-of-network distinction is built into every piece of plan communication. Members know to check provider directories. In an RBP plan, the equivalent guidance is to use the plan's pre-service advocacy line before scheduling non-emergency procedures.
This pre-service call does several things. The advocacy team confirms the provider's history with RBP reimbursement, alerts the member to any known balance billing risk at that facility, and if appropriate, identifies alternative providers with equivalent quality ratings who have a cleaner track record. For employers who invest in member education at enrollment, the pre-service call becomes routine within one or two plan years. For employers who under-communicate, it remains a friction point.
The employee communication piece is the most common reason RBP implementations struggle. The plans that work well invest in clear enrollment communication that explains the process, celebrates the access breadth, and makes the advocacy team phone number impossible to miss.
The cost advantage in reference-based pricing comes from two sources. First, claim-by-claim reimbursements are lower because the RBP schedule pays a defined multiple of Medicare rather than carrier-contracted rates. For employers in markets where carrier contracted rates run 250% or higher above Medicare, even a plan that pays at 150% of Medicare generates significant per-claim savings. Second, because the third-party administrator fee and stop-loss premium replace carrier overhead and profit margin, the administrative cost structure is often more transparent and competitive.
Across analyses of mid-size employer RBP adoptions, total plan cost reductions of 15% to 30% compared to prior-year fully insured premiums are commonly reported, with some groups achieving higher savings in markets with particularly elevated carrier rates. The Society for Human Resource Management and various benefits consulting firms have published case studies showing consistent savings in this range for well-designed implementations.
It is worth noting that these savings figures depend on actual claims experience. A group that has a high-cost claimant year in their first year on an RBP plan may see savings eroded by stop-loss premium increases in year two. The long-term savings case is stronger and more predictable for employers with three or more years of stable claims history. For a deeper look at how claims history drives your funding options, see What Your Group Health Plan's Loss Ratio Is Telling You.
Because reference-based pricing plans are self-funded, the employer needs stop-loss coverage to cap their exposure to catastrophic claims. Stop-loss in an RBP context works the same as in any self-funded arrangement. The specific stop-loss attachment point, the per-person threshold above which the stop-loss carrier takes over the claim, and the aggregate attachment point, the total claims threshold above which the stop-loss carrier covers the excess, are set at plan inception and directly affect the employer's risk profile.
Most RBP-compatible stop-loss carriers are familiar with the Medicare-anchored reimbursement model and price their coverage accordingly. The key item to verify when reviewing stop-loss proposals for an RBP plan is that the carrier's covered claims definition aligns with the plan's RBP reimbursement schedule, not with the provider's billed charges. Misalignment here has been a source of disputes in the early years of RBP growth, and most reputable third-party administrators and stop-loss brokers have developed language to address it. See How Stop-Loss Coverage Works in Self-Funded Health Plans for a full explanation of stop-loss mechanics.
Reference-based pricing is not universal in its fit. The employers who consistently report the best outcomes share a few characteristics. First, they have stable workforces with moderate turnover. High-turnover environments create continuous enrollment churn and make the member education investment harder to recoup. Second, they have workforces concentrated in markets where the provider landscape is competitive. Markets with one or two dominant health systems that control the bulk of local inpatient capacity tend to produce more balance billing friction. Third, they have leadership that is willing to communicate proactively with employees before, during, and after the switch. The plans that fail almost always fail because of inadequate member communication, not because of the reimbursement model itself.
Employers in industries with relatively predictable care patterns, such as professional services, technology, manufacturing, and distribution, often find RBP a natural fit. Employers with significant high-risk occupational health exposures may find that the stop-loss pricing reflects those exposures in ways that affect the anticipated savings.
Reference-based pricing is not the right answer for every employer. If your workforce is concentrated in a market dominated by one large health system with a strong local reputation, and that system is known to aggressively pursue balance billing, the member friction may outweigh the cost savings. If your workforce has strong preferences for specific providers and those providers are unlikely to accept RBP reimbursement without resistance, a network plan may deliver more satisfaction for a modest cost premium. If you are just starting your first health plan and have no prior claims history or benefits infrastructure, beginning with a simpler arrangement and migrating to RBP after one or two years of baseline data is often a more practical path.
For employers evaluating how RBP compares to level-funded alternatives, a side-by-side analysis is more useful than a conceptual discussion. See Level-Funded vs. Reference-Based Pricing for a direct comparison of how the two funding models compare across the dimensions that matter most to mid-size employers.
If you are considering reference-based pricing as a potential option at your next renewal, the most useful starting point is a claims analysis that shows your current effective reimbursement rates relative to Medicare. A good third-party administrator or benefits advisor can take your prior-year claims data and run a simulation showing what those same claims would have cost under a reference-based pricing schedule at various Medicare multipliers. That simulation tells you the theoretical savings before any implementation decisions are made.
The second evaluation step is a market assessment of your local provider landscape. Ask your advisor or third-party administrator how much balance billing activity they have seen in your specific region, and with which facilities. That data varies considerably by geography and is the single most important local factor in predicting how smooth the employee experience will be. A market where RBP plans have been running for three to five years and where most major providers have a track record of accepting reimbursement is very different from a market where RBP is newer and provider resistance is still higher.
Compare Funding Arrangements for Your Group
The Health Funding Projector lets you model reference-based pricing alongside level-funded, PEO, multiemployer trust, and fully insured options, side by side. Free, no login, no email gate. Built for employers with 20 to 250 employees.
Reference-based pricing is a health plan reimbursement model where the plan pays providers a set percentage above the Medicare reimbursement rate for each service, rather than paying rates negotiated with a carrier network. The Medicare rate serves as the transparent pricing anchor. Employees can use nearly any provider who accepts Medicare. Employers typically save 15% to 30% compared to a fully insured PPO plan because the RBP reimbursement is substantially lower than carrier-negotiated rates for the same services.
This is the balance billing scenario. When a provider receives the RBP payment and determines it is less than their expected rate, they may send the patient a separate bill. Well-designed RBP plans include an advocacy and legal support service that disputes these balance bills on behalf of members at no charge to the employee. Plans with a member hold-harmless provision take this a step further: the plan contractually guarantees the member will not owe any balance-billed amount beyond their normal cost-sharing, with the third-party administrator or plan handling the dispute. Before adopting an RBP plan, ask specifically how the plan handles balance billing and whether hold-harmless language is included in the plan document.
Not exactly. Reference-based pricing is a reimbursement methodology, and it is almost always implemented within a self-funded or partially self-funded plan structure. But self-funded plans can use carrier-negotiated network rates or other reimbursement models instead of RBP. Think of self-funding as the overall plan structure, where the employer bears the claim liability, and reference-based pricing as the method used to set reimbursement levels within that structure. Most RBP plans do require stop-loss coverage, which protects the employer from catastrophic individual or aggregate claims, the same as other self-funded arrangements.
Analyses across the mid-size employer segment consistently show total plan cost reductions of 15% to 30% compared to prior-year fully insured premiums when employers switch to well-designed RBP arrangements. Savings vary based on the carrier rates in your prior plan, your local market's provider balance-billing activity, and your group's own claims experience. The employers who see the highest savings tend to be in markets where carrier rates have historically run well above Medicare and where the RBP model has been operating long enough for provider acceptance to be well-established.
The most important habit to build is using the plan's pre-service advocacy line before scheduling any non-emergency procedure. That call takes five to ten minutes and lets the advocacy team verify the provider's track record with RBP reimbursement, identify any known balance billing risk at that facility, and when appropriate, suggest alternative providers of equal quality. For emergency care, there is no pre-service call required. For planned procedures like imaging, specialist consultations, and elective surgery, the pre-service call is the single most effective step an employee can take to avoid out-of-pocket surprises. Employers who make the advocacy line number visible and easy to reach in their employee materials see significantly smoother first-year experiences than those who bury it in the plan document.
This content is provided for educational purposes and does not constitute legal, tax, or benefits advice. Consult your compliance counsel and a licensed benefits advisor before making plan design decisions.
Sam Newland, CFP®, is the founder and president of PEO4YOU and Business Insurance Health. With more than 13 years in employee benefits and a background as a nationally ranked benefits advisor, Sam built PEO4YOU to give mid-size employers the same market access and transparency previously available only to large corporations. Contact: [email protected] | 857-255-9394
April 29, 2026

April 29, 2026
April 29, 2026
April 29, 2026
Recent Posts

April 29, 2026

April 29, 2026

April 29, 2026

April 29, 2026

April 28, 2026

April 28, 2026
Get In Touch— We’re available 24/7
"*" indicates required fields
“We respect your privacy. Your contact information will be used solely for the purpose of responding to your inquiry and will not be shared with third parties.”
Click To Open Modal
Get In Touch— We’re available 24/7
"*" indicates required fields
“We respect your privacy. Your contact information will be used solely for the purpose of responding to your inquiry and will not be shared with third parties.”
Thanks!
We will be in touch soon.
If you're looking to book a consultation now
Affordable health and benefits plans for small businesses, freelancers, and independent contractors.

Copyright © 2026. Peo4you. All rights reserved.