BCBS PPO National Network
| Deductible: | $1,000 |
| Coinsurance: | 80/20 |
| Out-of-Pocket: | $3,800 |
| Primary Care Co-pay: | $25 |
| Specialist Co-Pay: | $50 |
| Medications: | Generic 10%; Brand 35% (see SBC for more details) |
| Wellness & Teledoc Visits: | No Charge |
(In-network only)
See Health Plan Outline for More Details

Principal PPO Dental Network
| Annual deductible network | Coinsurance network pays | |
| Preventative | $0 | 100% |
| Basic | $50 | 80% |
| Major | $50 | 50% |
Max benefit: $2,000 per calendar year
New Benefit: Implant coverage (see SBC for details).
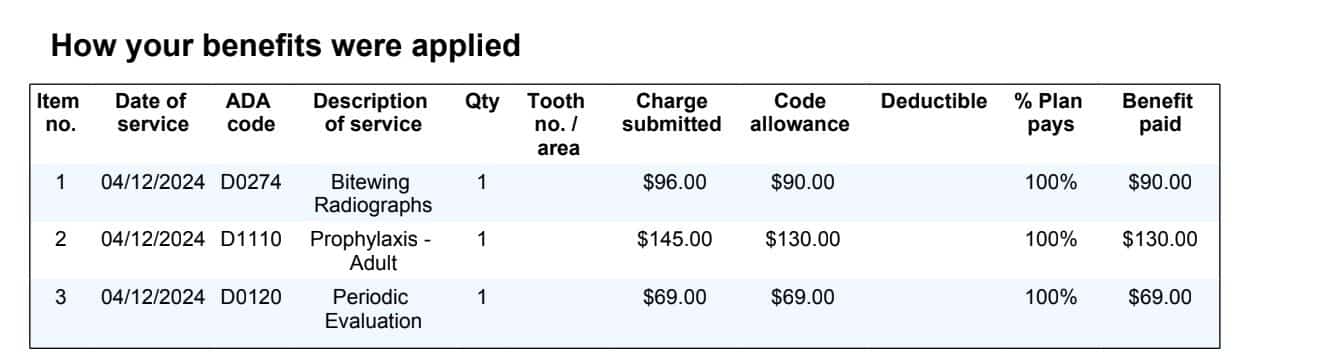
Out-of-Network Coverage Available (Click Here to See Claim Example)

VSP Vision
| Exams: $10 copay, 1 exam every 12 mo |
| Glasses: $25 copay for single lenses |
| Frames: Up to $250 every 24 mo |
| Contacts: Up to $250 every 12 mo |
At PEO4YOU, we believe comprehensive healthcare should be accessible, transparent, and tailored to your needs. That’s why every member receives a complete benefits package — medical, dental, vision, and life benefits — designed to give you peace of mind and real value.
BCBS PPO National Network
| Deductible: | $1,000 |
| Coinsurance: | 80/20 |
| Out-of-Pocket: | $3,800 |
| Primary Care Co-pay: | $25 |
| Specialist Co-Pay: | $50 |
| Medications: | Generic 10%; Brand 35% (see SBC for more details) |
| Wellness & Teledoc Visits: | No Charge |
(In-network only)
See Health Plan Outline for More Details
Principal PPO Dental Network
| Annual deductible network | Coinsurance network pays | |
| Preventative | $0 | 100% |
| Basic | $50 | 80% |
| Major | $50 | 50% |
Max benefit: $2,000 per calendar year
New Benefit: Implant coverage (see SBC for details).
Out-of-Network Coverage Available (Click Here to See Claim Example)
VSP Vision
| Exams: $10 copay, 1 exam every 12 mo |
| Glasses: $25 copay for single lenses |
| Frames: Up to $250 every 24 mo |
| Contacts: Up to $250 every 12 mo |

5 year average renewal of less than 3% – Trust established in 1958 – BCBS network since 2004 – Enrollment available year round – No underwriting
Features | H&W 125 | DENTAL 125 | VISION 125 | LIFE 10K | ADMIN125 | Union | Total |
|---|---|---|---|---|---|---|---|
Employee Only | $731.00 | $65.00 | $10.00 | $5.00 | $100.00 | $27.00 | $938.00 |
Employee + Spouse | $1,500.00 | $130.00 | $22.00 | $5.00 | $200.00 | $27.00 | $1,884.00 |
Employee + (Children) | $1,146.00 | $130.00 | $22.00 | $5.00 | $200.00 | $27.00 | $1,530.00 |
Employee + Family | $1,636.00 | $190.00 | $35.00 | $5.00 | $200.00 | $27.00 | $2,093.00 |
Waived Employees | $5.00 | $27.00 | $32 |
6 consecutive renewals of 3% or less – Trust established in 1958 – BCBS network since 2004 – Enrollment available year round
Features | H&W 125 | DENTAL 125 | VISION 125 | ACCIDENT | LIFE 10K | ADMIN125 | Union | Total |
|---|---|---|---|---|---|---|---|---|
Employee Only | $746.00 | $75.00 | $15.00 | $12.00 | $10.00 | $100.00 | $27.00 | $985.00 |
Employee + Spouse | $1,530.00 | $150.00 | $30.00 | $12.00 | $10.00 | $200.00 | $27.00 | $1,959.00 |
Employee + (Children) | $1,169.00 | $150.00 | $30.00 | $12.00 | $10.00 | $200.00 | $27.00 | $1,598.00 |
Employee + Family | $1,669.00 | $220.00 | $45.00 | $12.00 | $10.00 | $200.00 | $27.00 | $2,183.00 |
Waived Employees | $10.00 | $27.00 | $37 |

Accident coverage is for Employee/Member only
Groups above 10 have custom ancillary rates
First Year Dental Max is $1,000, Second year increases to $2,000
Surcharge for 4 or more dependent children – Dental :$50 , Vision: $15 per child.










Read how Clever has transformed productivity for our users
and hear their success stories.












Affordable health and benefits plans for small businesses, freelancers, and independent contractors.

Copyright © 2026. Peo4you. All rights reserved.