Every year, your health plan sends you a document called the Summary of Benefits and Coverage. It arrives during open enrollment, buried in a stack of PDFs or tucked inside a benefits portal you visit once a year. Most employers glance at the premium number, maybe check the deductible, and move on. That is a mistake that costs real money.
The SBC is the single most important document in your entire benefits program. It is a standardized, federally mandated disclosure that every health plan must provide in the same format, using the same definitions, with the same coverage examples. Yet according to the Kaiser Family Foundation's 2025 Employer Health Benefits Survey, fewer than 35% of small business owners report reading their SBC in detail before making plan decisions. The rest rely on their broker's summary or the carrier's marketing materials, both of which are designed to sell, not to inform.
This guide walks you through every section of the SBC and shows you how to use the document to make smarter plan decisions.
The Summary of Benefits and Coverage was created by the Affordable Care Act in 2010 and became mandatory for all health plans starting in 2012. The regulation (45 CFR 147.200) requires every group health plan and health plan issuer to provide a uniform summary of benefits in plain language, using a template developed by the Department of Health and Human Services.
The document is typically 8 pages long. It uses a standardized format with specific sections that appear in the same order on every SBC, regardless of carrier. This means that when you compare an Aetna PPO to a UnitedHealthcare EPO to a Blue Cross HMO, you are looking at the same categories, the same definitions, and the same coverage examples. No other document in the benefits world offers this level of comparability.
Under federal law, employers must provide the SBC to employees:
Failure to provide the SBC on time can result in penalties of up to $1,363 per failure (adjusted annually for inflation), per the Department of Labor's enforcement guidelines.
The top of page 1 identifies the plan name, coverage period, and contact information. This section seems straightforward, but it contains a detail most employers overlook: the coverage period dates. If your plan year runs January through December but your renewal effective date is March 1, you may have a mismatch between the SBC coverage period and your actual enrollment window. This matters because the SBC reflects the plan as it exists during the stated coverage period. If you are comparing a current plan SBC to a renewal offer, make sure you are comparing the same coverage period.
This is the section most people read. It contains four key numbers presented in a standardized grid:
| Question | What It Means | What to Watch For |
|---|---|---|
| What is the overall deductible? | The amount your employee pays before the plan starts covering services | Is it embedded or aggregate for family coverage? Embedded deductibles let individual family members meet their own threshold. |
| Are there services covered before the deductible? | Preventive care is always pre-deductible under ACA. Some plans also cover office visits and Rx before deductible. | Plans that cover primary care visits before the deductible have dramatically better employee satisfaction scores. |
| Are there other deductibles for specific services? | Some plans have separate pharmacy deductibles or out-of-network deductibles | A separate $500 pharmacy deductible on top of a $3,000 medical deductible means total exposure is $3,500 before coverage kicks in. |
| What is the out-of-pocket maximum? | The most your employee will pay in a year for covered services | For 2026, the federal limit is $9,450 individual / $18,900 family. Many plans set lower maximums. |
The out-of-pocket maximum is arguably the most important number on the SBC. Most employers fixate on the deductible, but the out-of-pocket maximum determines the worst-case scenario for an employee who has a serious health event. An employee diagnosed with cancer, requiring surgery and ongoing treatment, will blow through any deductible in weeks. What matters then is the out-of-pocket maximum: $5,000 vs. $9,450 is a $4,450 difference that can determine whether an employee faces financial hardship or manageable costs.
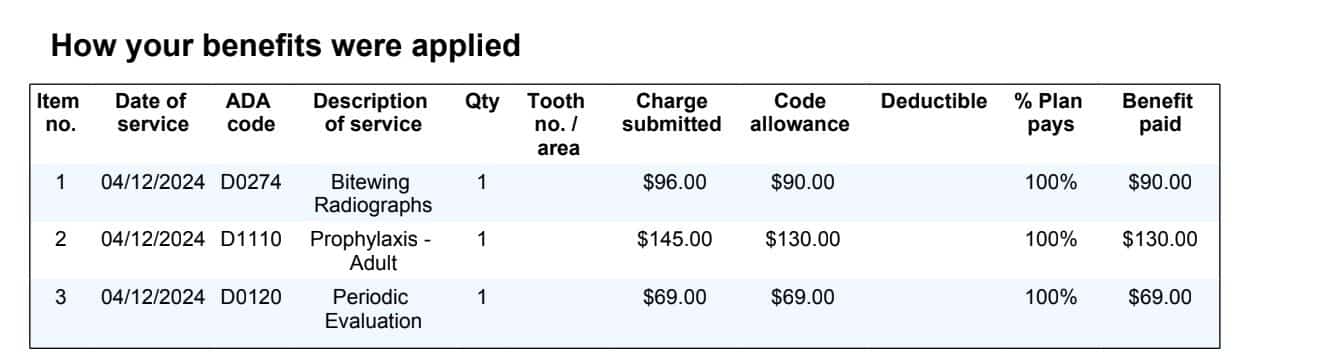
Pages 2 and 3 of the SBC contain the detailed benefits grid. This is where the plan lists how it covers specific services: primary care visits, specialist visits, diagnostic tests, imaging, outpatient surgery, hospital stays, emergency room visits, mental health services, prescription drugs, and rehabilitation.
For each service, the SBC shows three things:
This section is where you find the details that actually affect your employees' daily experience with their health plan. A $40 specialist copay vs. a $75 specialist copay might seem minor, but for an employee managing a chronic condition who sees a specialist monthly, that is a $420 annual difference per employee.
Page 4 contains two standardized coverage examples that every SBC must include:
These examples use standardized assumptions developed by HHS so that every plan calculates costs the same way. This is the closest thing to a real-world cost comparison that exists in the benefits world. Yet fewer than 20% of employers report using these examples when evaluating plans, according to a 2024 SHRM survey on benefits decision-making.
Here is why these examples matter: Two plans might both show a $2,000 deductible and $6,000 out-of-pocket maximum. But Plan A might estimate the diabetes patient's annual cost at $5,400 while Plan B estimates $3,800. That $1,600 difference comes from variations in copay structure, formulary tier placement for diabetes medications, and lab work coverage. The deductible and out-of-pocket maximum alone would never reveal this difference.
| Coverage Example | Plan A (PPO, $2,000 deductible) | Plan B (EPO, $2,000 deductible) | Difference |
|---|---|---|---|
| Managing Type 2 Diabetes | $5,400 estimated annual cost to patient | $3,800 estimated annual cost to patient | $1,600/year |
| Having a Baby (Normal Delivery) | $4,200 estimated cost to patient | $3,100 estimated cost to patient | $1,100/event |
If you have 25 employees and even 3-4 are managing diabetes, the plan choice difference is $4,800-$6,400 per year in employee out-of-pocket costs. That is money your employees feel directly, and it drives satisfaction and retention.
The SBC identifies the plan's network type, but it does not explain what that means in practice. Here is a clear breakdown:
| Network Type | Referral Required? | Out-of-Network Coverage? | Best For |
|---|---|---|---|
| HMO | Yes, for specialists | Emergency only | Cost-conscious employers; employees who prefer lower premiums and predictable copays |
| PPO | No | Yes, at higher cost | Employees who want flexibility; distributed workforces with employees in multiple states |
| EPO | No | No (except emergencies) | Balance of flexibility and cost savings; single-state or metro-area workforces |
| POS | Yes, for out-of-network | Yes, with referral and higher cost | Employers who want HMO savings with limited out-of-network access as a safety valve |
The network type decision has a ripple effect through the entire SBC. An HMO will generally show lower copays and lower premiums but restricts provider choice. A PPO will show higher premiums but gives employees the freedom to see any provider. For a 25-employee company, the premium difference between an HMO and a PPO can range from $1,200 to $3,600 per employee per year, according to KFF's 2025 survey data.
The SBC's prescription drug section lists cost-sharing by tier, but the tier structure itself is where the real costs hide. Most plans use a 4-tier or 5-tier formulary:
| Tier | What It Covers | Typical Cost to Employee | SBC Red Flag |
|---|---|---|---|
| Tier 1 (Generic) | Generic medications | $10-$20 copay | If generic copay exceeds $25, the plan is expensive |
| Tier 2 (Preferred Brand) | Brand-name drugs on the formulary | $30-$60 copay | Check if common medications (statins, blood pressure) are Tier 1 or Tier 2 |
| Tier 3 (Non-Preferred Brand) | Brand-name drugs not on the preferred list | $75-$150 copay or 30-50% coinsurance | If the plan uses coinsurance instead of copay, employee costs are unpredictable |
| Tier 4 (Specialty) | Biologics, specialty medications | $200-$500 copay or 20-50% coinsurance | Specialty tier coinsurance on a $5,000/month drug can mean $1,000-$2,500/month to the employee |
The SBC will not tell you which specific drugs are on which tier. That requires the plan's formulary document, which is separate. But the SBC does tell you the cost structure, and that alone reveals whether the plan is designed for typical medication users or is shifting significant pharmacy costs to employees.
According to the Mercer National Survey of Employer-Sponsored Health Plans (2025), pharmacy costs now represent 28-33% of total health plan spending for small employers. A plan with aggressive pharmacy cost-sharing (high copays, coinsurance-based specialty tiers) might have a lower premium but could create significant financial burdens for employees taking ongoing medications.
Near the end of the SBC is a section titled "Excluded Services and Other Covered Services." This section lists what the plan does not cover. Common exclusions include:
These exclusions are where most employee complaints originate. An employee who assumes their plan covers weight loss surgery discovers at the worst possible moment that it does not. An employee undergoing fertility treatment finds out their $15,000 IVF cycle is not covered. Reading the excluded services section before enrollment, not after a claim denial, is one of the most important things an employer can do to prevent employee dissatisfaction.
Here is a step-by-step process for using SBCs to make better plan decisions:
Step 1: Line up the SBCs side by side. Print or open them on separate screens. Because the format is standardized, every section aligns directly.
Step 2: Compare the coverage examples first. The diabetes and maternity examples give you the most realistic cost comparison. If one plan costs $1,500 more in the diabetes example, that difference is real and will affect your employees.
Step 3: Check the out-of-pocket maximum. Lower is better for employee protection. The difference between a $6,000 and $9,450 out-of-pocket maximum is the difference between manageable and devastating for an employee facing a major health event.
Step 4: Review pharmacy tiers. If your workforce skews older (40+), pharmacy costs will be a significant portion of their healthcare spending. Plans with lower pharmacy cost-sharing save your employees real money.
Step 5: Read the exclusions. If your workforce is predominantly female and of childbearing age, fertility coverage matters. If your workforce includes employees with chronic conditions, check whether the plan excludes specific treatments.
Step 6: Compare network adequacy. The SBC identifies the network type, but you need to check whether your employees' current doctors are in-network. A lower premium is worthless if your employees have to switch providers.
Compare different plan structures and see how changes to deductibles, copays, and network type affect total costs for both employer and employees. No login required. Free.
The premium is not on the SBC. It is a separate document. Employers often compare premiums without comparing SBCs, which means they are choosing plans based on sticker price without understanding what they are actually buying. A plan with a $50 lower monthly premium per employee might have a $2,000 higher deductible, which shifts $2,000 of cost to each employee. For a 25-employee company, that is $50,000 in shifted costs that the premium comparison did not reveal.
A $40 copay for a specialist visit means the employee pays exactly $40 regardless of the total charge. A 30% coinsurance for a specialist visit means the employee pays 30% of whatever the specialist charges. If the specialist charges $300, that is $90. If they charge $500, that is $150. Coinsurance creates unpredictable costs for employees, and the SBC makes this distinction clear if you read it carefully.
The Mental Health Parity and Addiction Equity Act requires that mental health benefits be no more restrictive than medical/surgical benefits. But parity applies to financial requirements and treatment limitations, not to the actual coverage level. The SBC should show the same copay structure for mental health office visits as for medical office visits. If the SBC shows a $40 copay for a primary care visit but $75 for a mental health visit, that may be a parity violation worth reporting to your state regulator.
At the end of the SBC, there are two yes/no questions about minimum essential coverage and minimum value. If either answer is "No," the plan may not satisfy ACA requirements, and your employees may face tax penalties. For employers with 50+ full-time equivalent employees, offering a plan that does not meet minimum value (covering at least 60% of total allowed costs) triggers potential employer shared responsibility penalties of $4,350 per full-time employee in 2026.
One of the less obvious advantages of working with a Professional Employer Organization is that PEOs typically offer multiple plan options from the same carrier network, all with standardized SBCs that are easy to compare. Because the PEO is the plan sponsor, they negotiate plan designs that address the most common pain points employers face: reasonable deductibles, embedded family deductibles, pre-deductible primary care, and competitive pharmacy tiers.
When you evaluate PEO plan options, you are comparing SBCs from plans that have already been vetted for competitive cost-sharing, network adequacy, and compliance. This eliminates the most time-consuming part of the SBC comparison process: filtering out plans with poor designs that look good on premium alone.
For employers managing benefits for the first time, PEOs also handle the SBC distribution requirement. They ensure every employee receives the SBC during open enrollment, maintain records of distribution, and update employees when plan changes occur mid-year. This compliance function alone can save small employers significant administrative time and penalty risk. If you are setting up benefits for the first time, understanding the SBC is the foundation of making a good plan choice.
Consider a real scenario: A 30-employee accounting firm in Maryland was renewing their health plan. Their broker presented two options, both with similar premiums. The employer was about to choose Option A because the premium was $12 per employee per month lower.
A closer SBC comparison revealed:
The $12/month premium savings on Option A ($4,320 annually for the company) would have been offset by $32,000 in additional out-of-pocket costs borne by employees across the plan year. The employer chose Option B, and employee satisfaction scores on their next survey increased by 18 points. As the data shows in our analysis of employee turnover costs, benefit satisfaction directly correlates with retention.
Your health plan carrier or benefits administrator is required to provide the SBC. Most carriers post SBCs on their employer portal. If you use a PEO, the SBC is typically available through the PEO's benefits enrollment platform. You can also request a copy directly from the carrier, and they must provide it within 7 business days.
No. The SBC is a standardized, 8-page summary designed for quick comparison. The SPD is a longer, more detailed document that covers all plan rules, claims procedures, and ERISA rights. The SBC is for comparison shopping; the SPD is for understanding the full legal terms of your plan. Both are required documents.
Yes. The Department of Labor can impose penalties of up to $1,363 per failure for willful failure to provide the SBC. Each employee who does not receive the SBC on time constitutes a separate failure. For a 25-employee company, that is a potential penalty of over $34,000.
The SBC must be updated and redistributed whenever there is a material modification to the plan during the plan year. At minimum, a new SBC is required at each annual renewal. If the plan changes mid-year (benefit modifications, carrier change, network change), a new SBC must be provided within 60 days of the change.
If you find discrepancies between the SBC and your actual plan experience, contact your carrier or benefits administrator immediately. Under federal law, the plan document (not the SBC) governs in the event of a conflict. However, if the SBC misstates a benefit and an employee relies on that misstatement, the employer or plan may face liability.
No. The SBC only covers medical (and sometimes integrated pharmacy) benefits. Dental and vision plans have their own disclosure documents. If your health plan includes embedded pediatric dental (as required by ACA for certain plans), that will appear in the SBC, but standalone dental and vision plans are separate.
Yes, and this is one of the SBC's most powerful features. Because Marketplace plans also use the same standardized SBC format, employees can directly compare their employer plan with individual Marketplace options. This is particularly useful for employees evaluating whether their employer's plan provides good value relative to subsidized Marketplace alternatives.
Sam Newland, CFP® has spent 13+ years in employee benefits consulting, helping small and mid-size employers navigate health plan decisions, funding strategies, and compliance requirements. As founder of PEO4YOU and Business Insurance Health, Sam specializes in translating complex benefits documents into actionable decisions that save employers money and improve employee satisfaction.
April 12, 2026

April 12, 2026
Recent Posts

April 12, 2026

April 12, 2026

April 11, 2026

April 11, 2026

April 10, 2026

April 10, 2026
Get In Touch— We’re available 24/7
"*" indicates required fields
“We respect your privacy. Your contact information will be used solely for the purpose of responding to your inquiry and will not be shared with third parties.”
Click To Open Modal
Get In Touch— We’re available 24/7
"*" indicates required fields
“We respect your privacy. Your contact information will be used solely for the purpose of responding to your inquiry and will not be shared with third parties.”
Thanks!
We will be in touch soon.
If you're looking to book a consultation now
Affordable health and benefits plans for small businesses, freelancers, and independent contractors.

Copyright © 2026. Peo4you. All rights reserved.